
DESIGN MANAGEMENT - CAPSTONE PROJECT
Improving Social and Academic Success Rates of College Students with Bipolar Disorder using a Strategic Design Intervention.
TEAM MEMBERS ARE:
Ben Ge | Layla Hassoun | Chuck Ruud | Yunhee Song | Kendall Veenema | Andrea Villarreal
Advisors: Denise Tahara + Edwin Kuo
The Challenge
Bipolar disease in college students is a critical public health issue and presents a significant challenge to college health services, faculty and the families of these young adults. In 2014, an estimated 1.7 million people age 18 to 25 were diagnosed with a serious mental disorder (SAMSHA, 2015). Students with bipolar disorder often bear the burden of stigma and social isolation which further facilitates a lack of sense of belonging with their college community and can impede help seeking behavior and engagement with mental health services. The National Alliance on Mental Illnesses (NAMI) 2012 survey report on mental health found that stigma remains the number one barrier to students accessing services and supports on campus among other barriers such as their busy schedule, limited hours of service, lack of information, and long appointment waitlists (NAMI, 2012). Colleges are overwhelmed by the increase of mental health related demands and there is no consistent, nationwide standard of mental health care on campuses (Wilson, 2015). The need for systematic improvements is timely as students with significant mental health problems have double the risk of departure from college (The Healthy Minds Network, 2013).
Communication, coordination and collaboration among stakeholders is needed now more than ever to connect students with on campus mental health services before they become distressed. This early intervention, or early engagement, is critical to the daily management of their mental illness and is a preventative measure to exacerbated symptoms. The platforms and outlets in which services communicate with students is key to creating authentic connections as younger generations are saturated with information.
Why we can make a DIFFERENCE
Science and technology have driven incredible innovation in healthcare. Preventive medicine, procedural advancements and humanized technologies such as the introduction of telehealth are just a few examples of how these innovations have brought a higher level of quality care for patients. Clinically, the US has never been so well equipped but with a continuously changing ecosystem and new demands from emerging generational challenges, systematically the healthcare sector must evolve to meet these growing needs and to continue to connect with younger patients through platforms they are receptive to.
Wired to look at challenges as opportunities of change, strategic designers use iterative processes to develop empathic communications, products, and services, and then test these theories and prototypes. We look holistically at the whole system and by making connections among all stakeholders involved, the design thinking process produces relevant, human-centered, closed loop solutions.
Healthcare is in a transitional period which presents an opportunity to bring design thinking approaches to research and databased processes. Applied to scientific and technological methodologies, design thinking can help reinvigorate the delivery of healthcare to meet the needs of younger generations and the new challenges presented by them.
We Believe we can identify and bring together the cross disciplinary teams to find a holistic solution.
Discover Phase
Methodology:
Using the 4D method – discover, define, design, deliver – we carefully studied the landscape of services on college campuses and through empathic modeling, studied the student with bipolar disorder.
Utilize research and findings, best practices and methodologies, medical and holistic interventions to inform the solution.
Develop the solution using an iterative process involving primary, secondary and anecdotal research with patients, their carers, families and health professionals.
Source the fine craft of design thinking: from empathy and observation to brainstorming and prototyping.
Research
On Campus status - While the increase in students accessing counseling services is broadly viewed as positive, our review of existing college health services found that most higher education institutions are currently unequipped to meet the growing mental health demand and to deliver the type of support systems that students with mental health disorders require. In some instances, this lack of infrastructure has led to discriminatory treatment and students in exasperated states of mania or depression “slipping through the cracks”. The number of students seeking counseling for “severe” psychological problems jumped from 16% in 2009 to 39% in 2012 (Baker, 2014). Survey data shows that with the rising number of students seeking care, 42% of mental health budgets stayed the same and 7% decreased (Baker, 2014). Most college campuses only allow 6 to 12 therapy visits per student per calendar year. A third of all college counseling centers consistently have appointment waitlists (Wilson, 2015, p. 39) and for a nonemergency visit, students are often waitlisted for up to a month (Domonell, 2013). In a recent survey completed by counselors at community colleges, the access to services was even less attainable as “only 8% of institutions provide onsite psychiatry” and “19% said no personal or mental health counseling was offered” at all (Patel, 2015, p. A45 and A47). This means that students must seek help off campus – which is not always easy – or go without care.
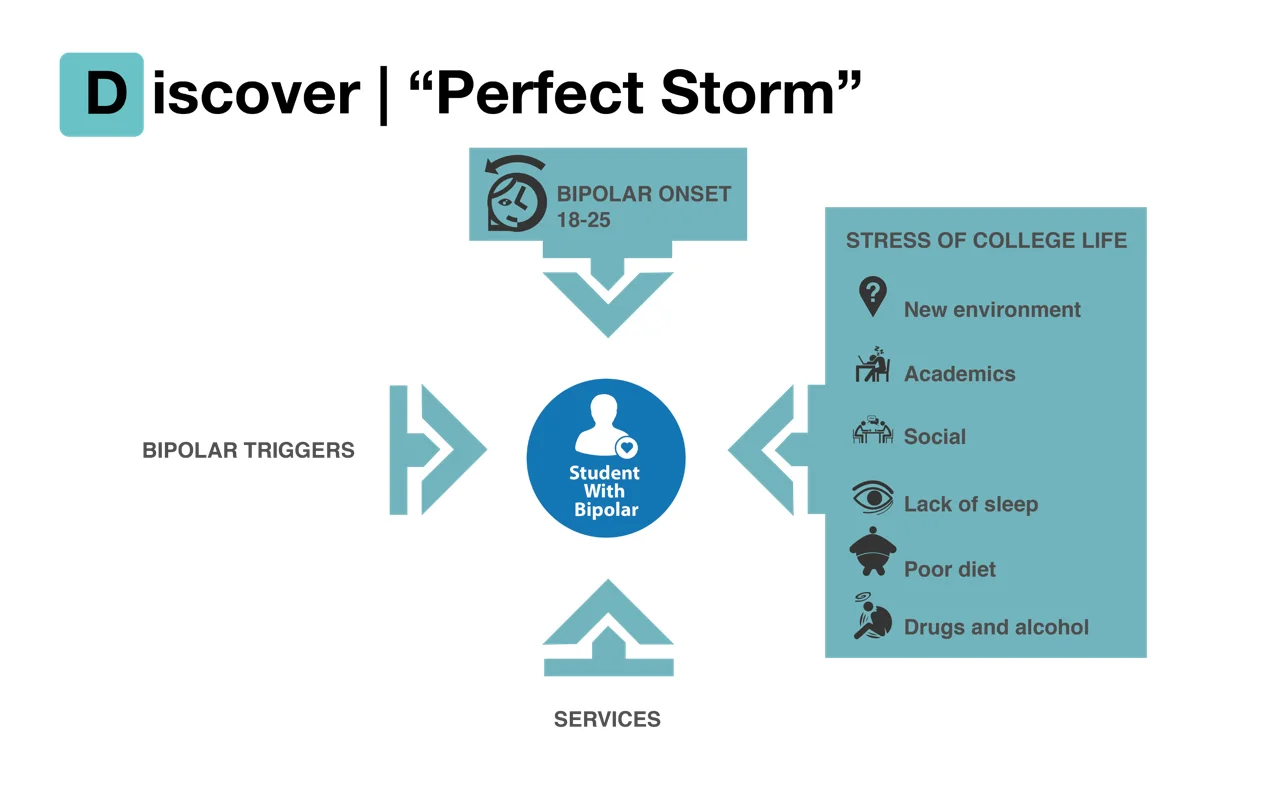
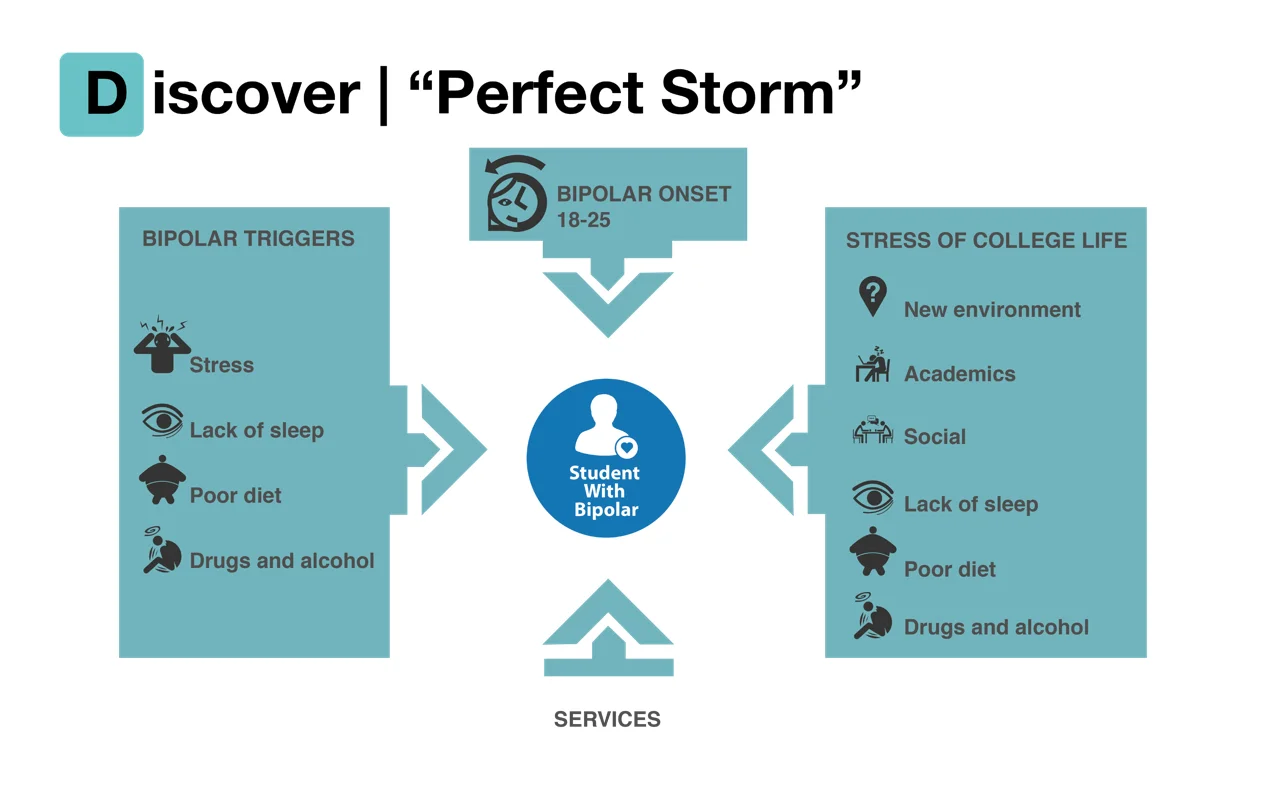
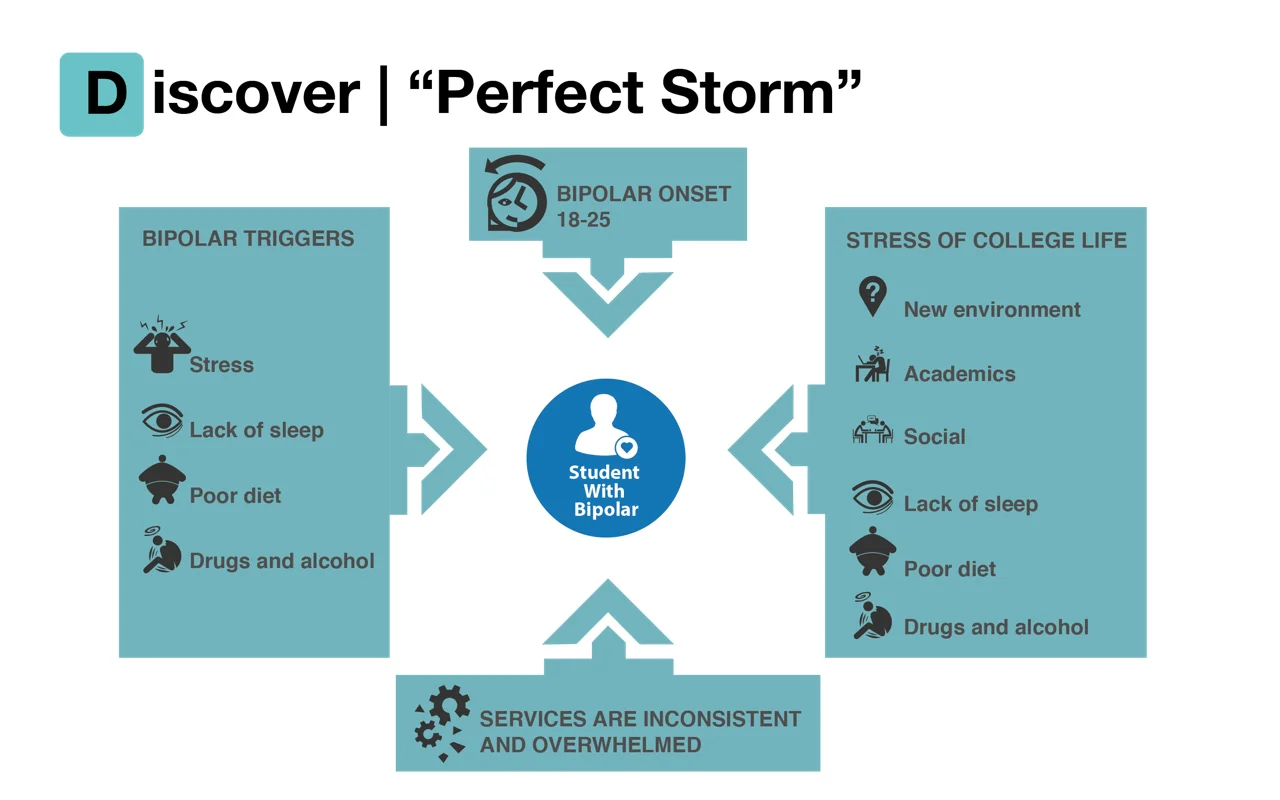
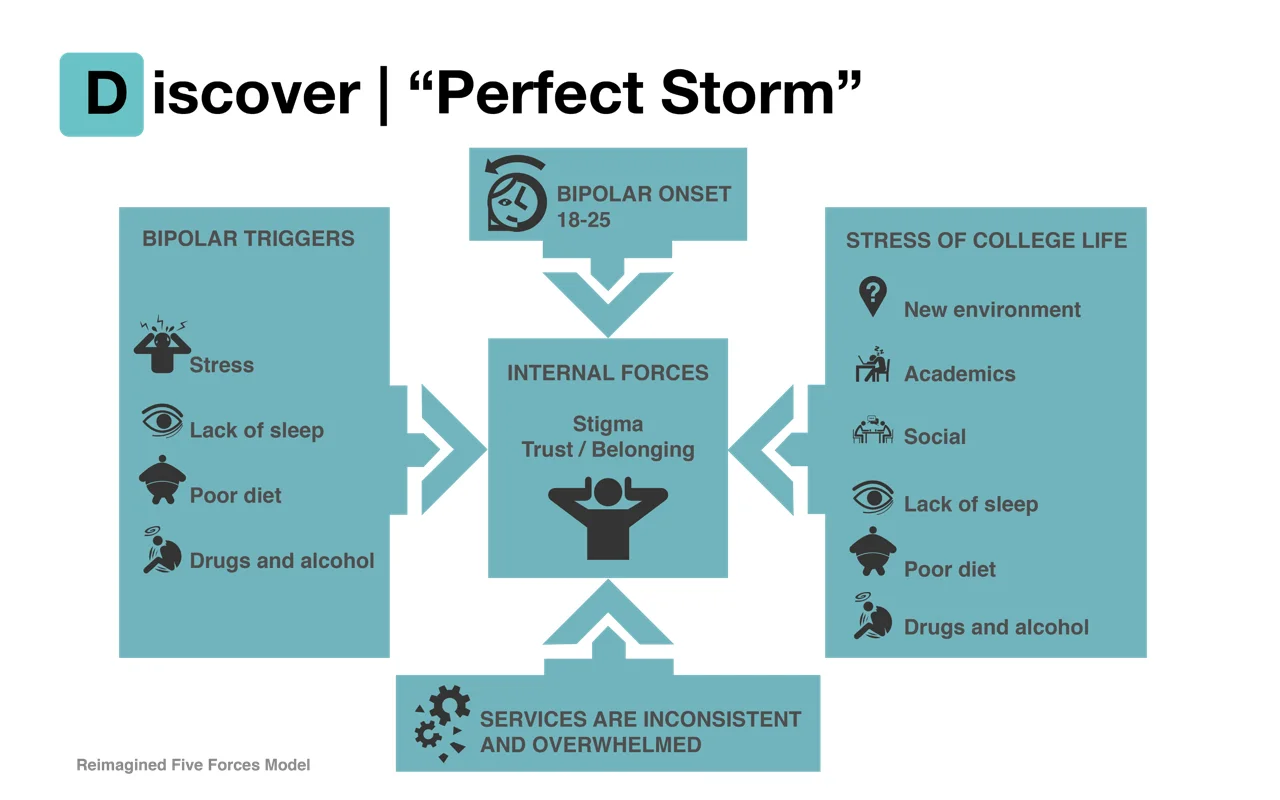
We found the students are going through a "perfect storm" of circumstances. These forces create triggers for episodes of ether a manic or depressive state and are barriers to getting help as they arrive on campuses.
Define phase
At the root cause, the existing problem is the lack of trust, authentic connection and engagement between the student and campus mental health services before the student becomes distressed and symptoms become exasperated so that when they are experiencing mania, depression or a state of psychosis, the relationship is established, trust exists and help seeking behavior is facilitated. While there may be short stints of interaction with on campus services, there is no consistent and sustained relationship that is critical to the students daily disease management throughout their entire college experience.
The problem isn’t necessarily in the students lack of knowledge about what mental health services are available, but rather in both the students initiative for help seeking due to extenuating external and internal factors and the formal services not being readily available in moments of crisis . With college health services overwhelmed by growing mental health demands and one third of all counseling centers consistently on appointment waitlists (Wilson, 2015, p. 39), the formal system is becoming drained.
User Needs:
Emotional Needs: Trust; Stigma; Sense of Belonging
Behavioral Needs: Daily Medication; Therapy; Self Awareness for help seeking behaviors
System Gaps:
Over capacity; No consistent daily integration with the students?
Key Insights:
- Primary research and analysis of 13 colleges.
- Cross referenced the 13 college analysis with the Jed/Clinton Foundation Framework
- Discovered opportunities






Design phase
Solution:
So where is the opportunity to create trust, an authentic connection and daily engagement between the student and college mental health services? Looking at the existing “supports and services” journey of the student with bipolar disorder, we found that their support structure can be mapped out through four quadrants.
Their support structure starts with family and friends at home ( i.e., 1. ‘informal off campus’). Before the student arrives on campus, more often than not, they have interacted with a variety of mental health professionals that fall under 2. ‘formal off campus’ services. Once they arrive on campus, college health services or CAPS programs offered by the university are available to them, which are defined as campus baseline services in 3. ‘formal on campus’ quadrant. While many universities provide ‘informal oncampus’ services for additional support in student’s day to day life, such as RA’s, they are not utilized to their full service potential.
This capstone is to propose increasing the linkage of integrative services to give more value to the informal people, groups, and interactive technology that surround the student in their daily lives. This will be done by achieving:
● Help with daily disease management ( i.e., early intervention);
● The facilitation of day to day activities; Creating social capital/social success through life balancing group activities;
● Decreasing stigma and increasing trust;
● Facilitating ‘the why’ that drives help seeking behavior;
● Writing strategic plans for the role of informal people and groups; and
● Solidifying the link of ‘informal on campus’ services to ‘formal on campus’ services.
Opportunity has been identified to utilize ‘informal’ service stakeholders in the front line of communication, connection and engagement with students. Through an early intervention framework of both physical and digital touchpoints that the student is receptive to and can easily interact with, the ‘in the field’ informal services will help the overall system meet the student's emotional needs (trust, stigma, belonging) and actionable needs (adhering to daily medication, attending therapy sessions, developing self awareness) by way of continuum phases of early engagement, connect, engage, and sustain which are strategically delivered at critical times during their college experience. By layering these services together, it is our goal to create a community of support for the student and multiple opportunities to reinforce healthy habits.
By redesigning the context of the conversation to connect with the student in an environment that doesn’t isolate or stigmatize them means creating social capital or a sense of belonging within an approachable community which, as represented above, simultaneously provides them with a structured system of both formal and informal support without the student feeling like a patient. Social capital is defined as the networks of relationships among people who live and work in a particular society, enabling that society to function effectively. A recent article in the Journal of College Student Development, A Sense of Belonging Among College Students with Disabilities, reports on higher education research and narratives from students with invisible disabilities suggesting that the development of a sense of belonging is key to academic motivation, success and persistence in the postsecondary realm (Vaccaro, Daly Cano, & Newman, 2015). On campus informal services is a supplementary group very consistent in students daily lives, and when more formally integrated with on campus formal services, it is our hypothesis that these informal physical and digital connections can create the social capital for students with bipolar disorder that drives life balancing actions and help seeking behavior.




Delivery

Video production by Ben Ge, Voice over by Layla Hassoun and Graphics by Ben Ge and Chuck Ruud